shumayou@hotmail.com
09674342789
Patients with neck and/or arm Pain should be evaluated for issues with the neck (cervical spine). The cervical spine is made up of 7 vertebrae. The spinal cord runs through the middle of the cervical spine. Individual nerve roots exit the spinal cord at each cervical level. Compression of either the spinal cord or the nerve roots can result in neck Pain, arm Pain, tingling, numbness, and/or weakness. This often occurs due to a disc herniation or stenosis (thickened ligament). Severe compression of the spinal cord can result in upper arm and leg weakness, poor hand grip, dropping objects from the hands, loss of fine motor skills in the hands, and/or loss of balance. This constellation of symptoms is often referred to as cervical myelopathy. Patients may also experience Pain due to arthritic changes in the neck, resulting in facet hypertrophy or kyphotic alignment of the cervical spine.
Evaluation of neck/arm Pain includes a clinical exam, cervical x-rays, MRI scan, and possibly a CT scan.
Surgical treatments for neck/arm Pain are determined on an individual basis.
Treatment options include:
 Cervical ADR stands for artificial disc replacement in the cervical spine. It is a motion preservation technique that allows for decompression of the spinal cord and nerve roots and maintains the natural movement of the neck. It is usually indicated for patients with intractable neck and arm pain with disc degeneration, stenosis or a disc herniation.
Cervical ADR stands for artificial disc replacement in the cervical spine. It is a motion preservation technique that allows for decompression of the spinal cord and nerve roots and maintains the natural movement of the neck. It is usually indicated for patients with intractable neck and arm pain with disc degeneration, stenosis or a disc herniation.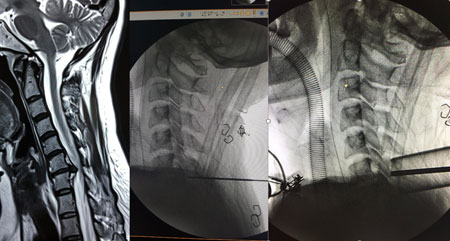 Posterior Cervical Decompression refers to several techniques that decompress the spinal cord and cervical nerve roots from a posterior approach. Such techniques include cervical foraminotomy, cervical laminectomy, and cervical laminoplasty. These techniques are usually indicated for patients with intractable neck and arm pain with stenosis, disc herniation, and/or compression of the spinal cord.
Posterior Cervical Decompression refers to several techniques that decompress the spinal cord and cervical nerve roots from a posterior approach. Such techniques include cervical foraminotomy, cervical laminectomy, and cervical laminoplasty. These techniques are usually indicated for patients with intractable neck and arm pain with stenosis, disc herniation, and/or compression of the spinal cord. Cervical PSF stands for posterior instrumentation and fusion of the cervical spine. It is a type of spinal fusion that stabilizes the spine from a posterior approach. It is sometimes associated with a posterior cervical decompression, such as a cervical laminectomy or foraminotomy, to relieve stenosis or pressure on the spinal cord. It is usually indicated for patients with intractable neck and arm pain with stenosis, kyphosis, and/or instability of the spine.
Cervical PSF stands for posterior instrumentation and fusion of the cervical spine. It is a type of spinal fusion that stabilizes the spine from a posterior approach. It is sometimes associated with a posterior cervical decompression, such as a cervical laminectomy or foraminotomy, to relieve stenosis or pressure on the spinal cord. It is usually indicated for patients with intractable neck and arm pain with stenosis, kyphosis, and/or instability of the spine.
Patients with back and/or leg pain should be evaluated for issues with the back (thoracic or lumbar spine). The thoracic spine is made up of 12 vertebrae and the lumbar spine is made up of 5 vertebrae. The spinal cord runs through the middle of the thoracic spine and ends around T12-L1. The spinal canal extends down to the sacrum and houses individual nerve roots. These individual nerve roots exit the spinal canal at each lumbar level. Compression of either the spinal cord/canal or the nerve roots can result in back pain, leg pain, tingling, numbness, and/or weakness. This often occurs due to a disc herniation, stenosis (thickened ligament), or instability of the spine such as with spondylolisthesis, scoliosis, or kyphosis. Severe compression of the spinal cord in the thoracic spine can result in leg weakness and/or loss of balance.
Evaluation of back/leg pain includes a clinical exam, lumbar x-rays, MRI scan, and possibly a CT scan and/or standing scoliosis x-rays.
Surgical treatments for back/ leg pain are determined on an individual basis.
Treatment options include:
 Lateral LIF is a type of spinal fusion that decompresses nerves and stabilizes the spine from a lateral approach. DLIF stands for direct lateral interbody fusion and XLIF stands for extreme lateral interbody fusion. It is usually indicated for patients with intractable back and leg pain with scoliosis, kyphosis, flat back syndrome, multiple level stenosis or degeneration, and/or instability of the spine.
Lateral LIF is a type of spinal fusion that decompresses nerves and stabilizes the spine from a lateral approach. DLIF stands for direct lateral interbody fusion and XLIF stands for extreme lateral interbody fusion. It is usually indicated for patients with intractable back and leg pain with scoliosis, kyphosis, flat back syndrome, multiple level stenosis or degeneration, and/or instability of the spine. 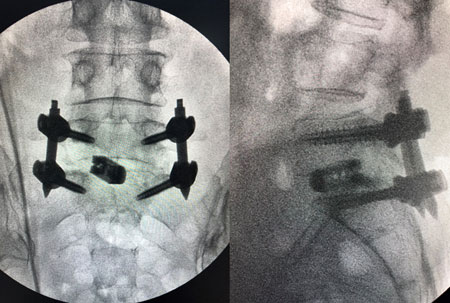 TLIF stands for transforaminal lumbar interbody fusion. It is a type of spinal fusion that decompresses nerves and stabilizes the spine from a posterior approach. It is usually indicated for patients with intractable back and leg pain with stenosis, disc herniation, and/or instability of the spine. Dr. Dutta specializes in minimally invasive TLIFs.
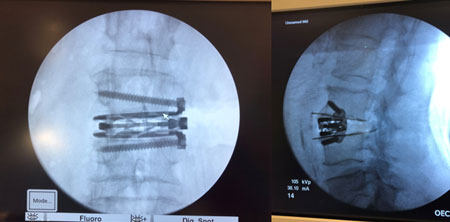
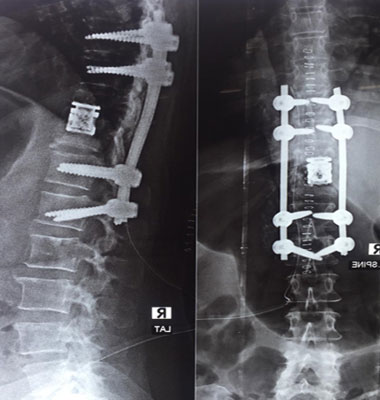
TLIF stands for transforaminal lumbar interbody fusion. It is a type of spinal fusion that decompresses nerves and stabilizes the spine from a posterior approach. It is usually indicated for patients with intractable back and leg pain with stenosis, disc herniation, and/or instability of the spine. Dr. Dutta specializes in minimally invasive TLIFs.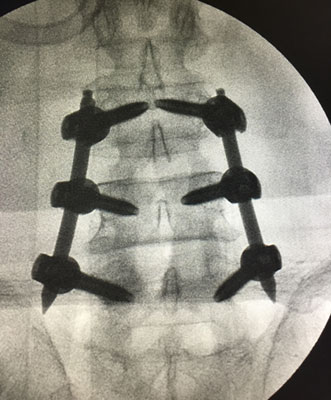 The goal of a posterior instrumentation and fusion is to stabilize the spine, reduce the curvature, and preserve the alignment. This is achieved with a pedicle screw and rod system, which is implanted using a minimally invasive approach. Multiple small incisions are made on the back, through which dilating tubes are placed. The screws and rods are passed through tubes so as to preserve the muscle attachments, contributing to the minimally invasive approach. The surgeon corrects the curve and alignment of the spine as he locks the rods into place. By using this minimally invasive approach, patients do not need to go to ICU, lose less blood/require fewer blood transfusions, and recover much faster, allowing them to get back to their daily activities sooner.
The goal of a posterior instrumentation and fusion is to stabilize the spine, reduce the curvature, and preserve the alignment. This is achieved with a pedicle screw and rod system, which is implanted using a minimally invasive approach. Multiple small incisions are made on the back, through which dilating tubes are placed. The screws and rods are passed through tubes so as to preserve the muscle attachments, contributing to the minimally invasive approach. The surgeon corrects the curve and alignment of the spine as he locks the rods into place. By using this minimally invasive approach, patients do not need to go to ICU, lose less blood/require fewer blood transfusions, and recover much faster, allowing them to get back to their daily activities sooner.
 Dr. Dutta handles all types of spine trauma both in the acute setting as well as chronic issues associated with spine trauma.
Dr. Dutta handles all types of spine trauma both in the acute setting as well as chronic issues associated with spine trauma.
Spinal Trauma begins with evaluation of the nature of spinal injury with emphases on the neurological status and the stability of the spine. The main goal is to maintain and preserve neurological function and at the same time provide for a stable spine. Spine surgeons tend to classify spinal injuries based on various parameters, most important being the above two.
Assessment of spinal trauma usually includes a thorough neurological exam, Xrays, Trauma CT Scan and MRI as needed. Once the nature and severity of the injury is established, surgery may include decompression and posterior stabilization, and/or Anterior corpectomy and/or combined anterior - posterior surgeries.
Dr. Dutta tries to use minimally invasive techniques to stabilize the spine anytime it is possible which includes Lateral LIF, Minimally invasive corpectomies, minimally invasive posterior stabilization and fusion. In the cervical spine anterior approaches such as ACDF may also be performed besides posterior fusion.
Spinal tumors can present as primary tumors or as metastatic tumors. They can be benign or cancerous. Invasion of bone by a tumor can result in fracture of the bone. Tumors can also evolve within the spinal canal or along a nerve root. Treatment of spinal tumors is determined based on the type of tumor, the presence of lesions in other parts of the body, the patient’s neurologic status, and the patient’s spinal alignment. If surgical intervention is indicated, the goal of surgery is to decompress the nerves and stabilize the spine.
 Infection of the spine can result in bony abnormalities, instability of the spine, poor spinal alignment, and nerve compression. Sometimes infection can be treated with antibiotics. More extensive cases are treated with surgical decompression and stabilization.
Infection of the spine can result in bony abnormalities, instability of the spine, poor spinal alignment, and nerve compression. Sometimes infection can be treated with antibiotics. More extensive cases are treated with surgical decompression and stabilization.
Office Address
68/c Hazra Road, 1st floor
Ballygunge,
Kolkata, West Bengal
shumayou@hotmail.com
09674342789
Follow Us

![]()


Copyright © 2017. All right reserved.